

 Kamanthi Wickramasinghe
Kamanthi Wickramasinghe Reply To:
Name - Reply Comment
Whenever there is a death caused by suicide it gives a reminder that there is a larger problem than the mere statistic it produces that needs to be addressed

Rights activists gather in Colombo and conduct a walk highlighting the need to prevent suicide from taking place
Every time a life is lost to suicide, it indicates a collective failure within the system. In Sri Lanka, a death by suicide is another statistic, but it points to a larger problem that needs to be addressed. While there is no one single factor that could trigger suicidal thoughts in individuals, a spate of incidents over the past few months, particularly with regards to youth suicides, paint a different picture.
Reported incidents in 2025
Some of the notable cases include the incident of a university student from Sabaragamuwa University followed by the Kotahena child’s incident which triggered a public outcry. A 13-year old boy from Ambalangoda succumbed to suicide in May. In early June a female student pursuing a Higher National Diploma at the Kuliyapitiya Technical College reportedly jumped into a lake in a case of attempted suicide. Thereafter three senior students and one female student were arrested in connection to the incident. Investigations revealed that the student attempted to take her own life due to a ragging incident. Investigations with regards to other three cases are still ongoing.
Global School-Based Student Health Survey
The Global school-based student health survey (GSHS) recommended by the World Health Organisation (WHO) is a collaborative surveillance project designed to help countries measure and assess the behavioural risk factors and protective factors in 10 key areas among young people aged 13 to 17 years. The 2024 GSHS Survey included a sample of students from Grades 8-12 in 40 government schools from across the country.
The 2024 survey is the third of its kind conducted by the Family Health Bureau and Ministry of Education, Higher Education and Vocational Education assessed health-related practices regarding dietary habits, physical activity, hygiene, mental health, oral health, substance use, violence, injuries, engagement with parents and peers and sexual behaviour among students in government schools.
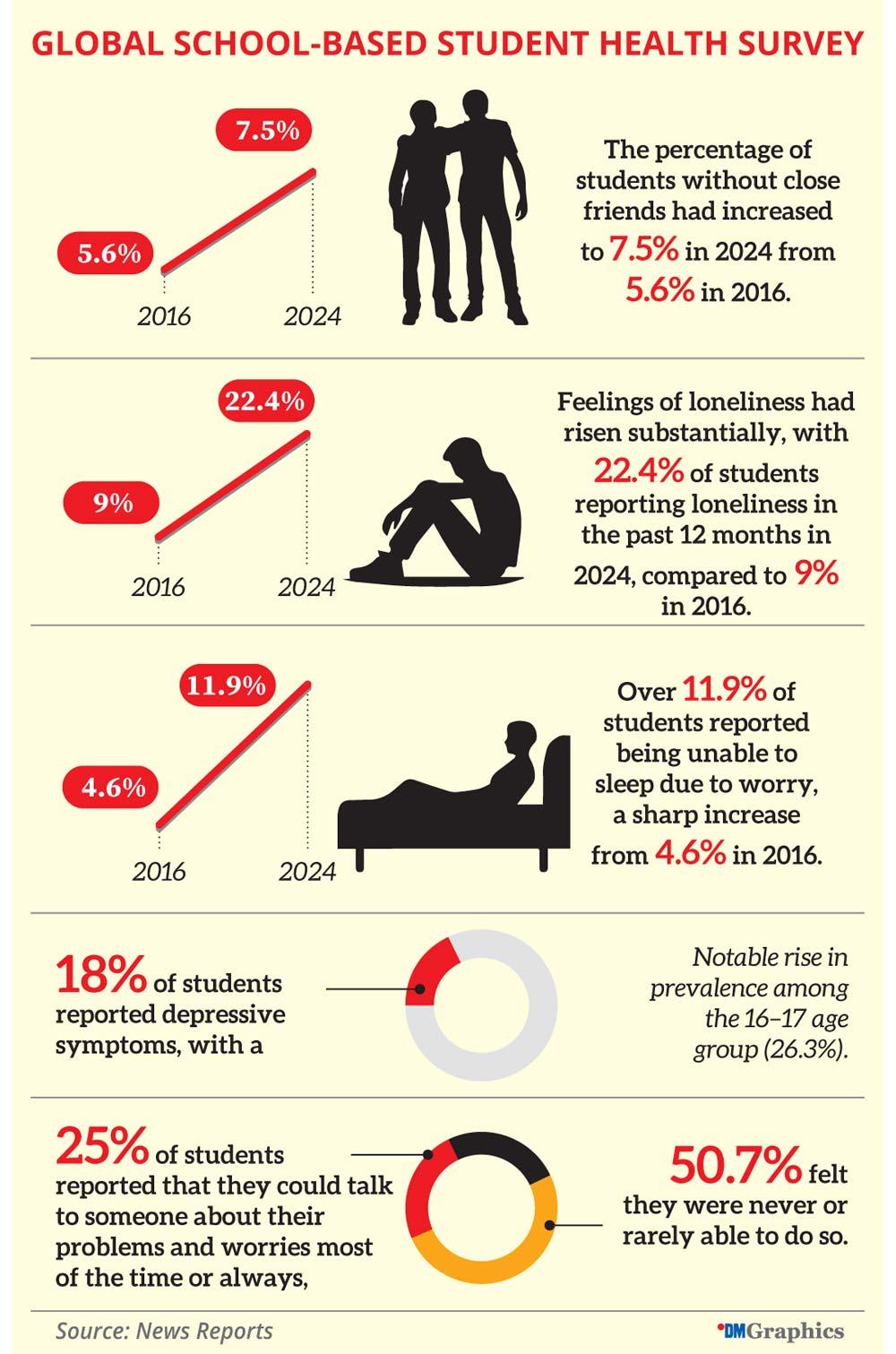
Critical trends and concerns in the mental health and psychosocial well-being of adolescents were observed in 2024, as compared to 2016. The percentage of students without close friends had increased to 7.5% in 2024 from 5.6% in 2016. Feelings of loneliness had risen substantially, with 22.4% of students reporting loneliness in the past 12 months in 2024, compared to 9% in 2016. Over 11.9% of students reported being unable to sleep due to worry, a sharp increase from 4.6% in 2016. Further, 18% of students reported depressive symptoms, with a notable rise in prevalence among the 16–17 age group (26.3%).
Only 25% of students reported that they could talk to someone about their problems and worries most of the time or always, while 50.7% felt they were never or rarely able to do so. The ability to talk to adults at school, such as teachers or counsellors, was particularly low, with just 7.9% reporting comfort in doing so, and 80.4% stating they rarely or never could.
During the course of 12 months in 2024, 2.1% of students reported seeking help from an adolescent clinic (Yowun Piyasa) during extremely difficult situations among students who have faced challenging situations. This was significantly better among males at 3.6%, compared to females (1%). Among the 13 to 15 age group, the percentage was 2.7%, compared to just 1.1% in the 16 to 17 age group.
The survey notes that the increasing trend in suicidal ideation and actual attempts could be attributed several inter-related factors. Firstly, heightened academic stress is a significant contributor, compounded by the potential misuse of addictive substances among students. Additionally, mass media and social media play a critical role in this issue; they often report on incidents involving mental health crises in dramatic fashion, which can influence public perception and individual behaviour. Furthermore, topics such as suicide attempts, negative family dynamics, and problematic relationships between parents and children have emerged as prevalent concerns. Lastly, the lingering effects of the COVID-19 pandemic cannot be overlooked. The shift to online learning has increased isolation for many students, diminishing opportunities for social interaction with peers and teachers that typically occur in physical classroom settings. These factors create a complex environment that may explain the troubling trends observed in 2024.
The findings of the GSHS 2024 highlight the urgent need for a comprehensive, multi-dimensional approach to address the numerous challenges Sri Lankan adolescents face. The survey underscored the urgent need to strengthen adolescent-focused programs and interventions within the broader Universal Health Coverage (UHC) framework and the need to institutionalize health education as an integral part of the curriculum.
Another observation included prioritising on the strengthening of adolescent-responsive health systems. This includes increasing resource allocation, making all health service providers aware on providing health services in an adolescent friendly manner, expanding access to adolescent-friendly health services, and creating widespread awareness of these services among adolescents and school children.
Helplines for those in need
1926 National Mental Health Helpline is a service available island wide and you can speak in either Sinhala, Tamil or English. An SMS service is also available from 8.00am-4.00pm.
With over 50 years of service in listening and befriending Sri Lanka Sumithrayo is an Organisation with a mission to prevent suicides and provide emotional support for those in need. Call 0707308308 or send a WhatsApp message on 0767520620.
CCC Line 1333 provides confidential and free support over the phone 24/7.
In all of the above helplines, callers can choose to be anonymous and each Organisation assures that your information will remain confidential.
 |
| Dr. Duleeka Knipe |
In this backdrop the Daily Mirror spoke to Dr. Duleeka Knipe, Associate Professor of Global Mental Health and Bristol Medical School’s Deputy Research Director for Equality, Diversion and Inclusion (EDI) on the trends, challenges and interventions that need to be sought to prevent youth suicides in Sri Lanka and the South Asian context. Dr. Knipe is a crusader against self-harm, conducting research and working passionately to provide evidence-based facts and figures to bring about effective preventive interventions, not just in Sri Lanka, but across the world. In 2019 she was presented with the prestigious De Leo Fund Award of the International Association of Suicide Prevention (IASP) in recognition of her “outstanding research into suicide prevention in low-and middle-income countries”.
Excerpts of the interview done with Dr. Knipe:
QWhat are some of the main factors that contribute to youth suicide in the South Asian context in this day and age?
Suicide is a devastating outcome, and the challenge we have is that there is never one clear reason why someone ends his/her life. There are likely to be an interplay of a number of different factors. Some of the research evidence points to the importance of family conflicts and ‘shame’ as important driver for self-harm. In South Asia and more globally there is concern over the role of media, in particular social media in self-harm behaviour in young people. The exact way in which this plays out though is not clear.
QSri Lanka has witnessed an alarming trend of youth suicide despite various awareness campaigns etc. What are your observations?
The evidence does not point to a rise in suicide rates in young people in Sri Lanka over any other age group. There is a rise in male suicide deaths overall and this is being driven by suicide by a particular method - this rise in this method however is seen across all age groups. I do note, however, that the public perception of this rise is probably higher than a real rise in rates.
QWhat sort of contribution do parents, teachers and peers have in this regard, in attempting to save the life of a child, student or friend?
Young people in Sri Lanka have been brought up with a set of social norms. Verbalising or expressing distress isn’t socially acceptable, particularly for young women. Self-harm often results and can be used as a tool for communication strategies to support healthy expression of distress could be really powerful. Having someone who understands and listens to you (and this is not restricted to Sri Lanka) is very important.
QThere is still a taboo around mental health, discussing issues with others and seeking access to mental health services. What more needs to be done in this regard?
As I said before, I think improving the communication skills in general terms is a really important area of work. In countries like Sri Lanka, mental illness doesn’t seem to always be associated with suicide or self-harm. It’s more mental distress. This distress could be reduced by increasing a person’s access to social capital as well as formal help. Schools are a great place to provide some of this support, by helping develop problem solving skills as well as being a point of contact and connection for young people. Schools are also a really important place to learn about things outside of academic subjects, such as what healthy relationships look like and future family planning.
QWhat are some immediate interventions that are required at state level to reduce youth suicides?
There isn’t real evidence to support a championing of an immediate intervention for youth suicides in Sri Lanka. However, optimising the school environment to shape the future generations to have the skills and resilience to deal with future problems is a promising area for future work. This would require trained and resourced staff, but also a recognition that academic achievement in of itself is unlikely to be the only output that should be important for schools and young people.














