Reply To:
Name - Reply Comment
Last Updated : 2024-04-24 22:26:00
12 January 2021 12:10 am - 1 - {{hitsCtrl.values.hits}}

 A healthcare worker receives the Pfizer-BioNTech COVID-19 vaccine at the Tor Verrgata hospital in Rome (AFP)
A healthcare worker receives the Pfizer-BioNTech COVID-19 vaccine at the Tor Verrgata hospital in Rome (AFP)
 As the world awaits the distribution of vaccines to speed up immunity against COVID-19, newer viral strains and mutations have left people in doubt.
As the world awaits the distribution of vaccines to speed up immunity against COVID-19, newer viral strains and mutations have left people in doubt.
However, medical experts are yet to conclude on the severity of new viral strains and whether they have the ability to escape vaccine immunity. But for Sri Lanka, an increase in testing and effective control policies seem to be the most viable option given the economic backdrop. Affordability of the vaccine, availability of cold storage facilities, side effects such as anaphylaxis and whether a new vaccine is needed for every emerging strain like in the case of influenza are further doubts that need to be cleared.
Emergence of mutations
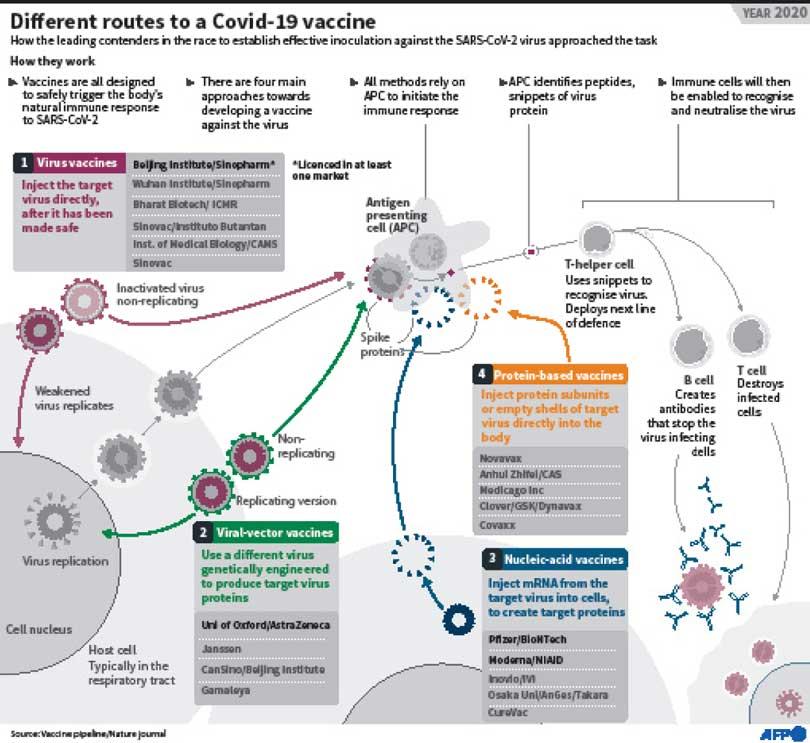
Speaking at a webinar organised by the College of Community Physicians to update the public on the pandemic situation, Chair Professor - Department of Microbiology at the Hong Kong University’s Faculty of Medicine and clinical and public health virologist Prof. Malik Pieris said that the SARS-Cov-2 virus is a RNA virus, the spikes get attached to the cell, the virus gets in and replicates inside the cell. “Without a living cell there’s no living virus. Once the virus enters, it starts making viral proteins and replicating RNA. These two together produce viral particles. In this phase when RNA viruses are copying there are errors. The whole genome is around 30,000 nucleotides and most mutations are bad for the virus and we don’t see them. Some of them survive, but may not make much of a difference to the virus. We are worried about a mutation when they change the property of the virus, for example the capacity to transmit or increase capacity to cause disease and now of course, escape vaccine. The primary driver for the virus is transmission,” said Prof. Pieris.
He said that the virus has undergone diversification through the mutation process. “Through the early viruses and as it spread worldwide there’s more diversity. It’s more like a family tree. The first mutation that was of biological significance was D614G in the spike protein. Once this mutation arose more viruses across the world have got it. The most likely explanation is that viruses with this mutation have a better fitness for transmission. Globally most of the viruses worldwide are viruses with this mutation that have essentially displaced 614D very likely due to increased transmission fitness,” explained Prof. Pieris.

Through the early viruses and as it spread worldwide there’s more diversity. It’s more like a family tree. The first mutation that was of biological significance was D614G in the spike protein. Once this mutation arose more viruses across the world have got it
Prof. Malik Pieris
Recent mutations – UK and South Africa
Two recent mutations are those found in UK and South Africa. “Both lineages share one particular mutation in common (S501Y) also in the spike chain along with other mutations in the spike chain. Even though it’s a common mutation they have arisen separately,” he added.
UK lineage:According to him, this lineage has acquired 23 mutations including in spike. “But how can rapid mutations occur? A virus can persist in an immunocompromised patient and such viruses acquire a lot of mutations in the same patient. It has a number of mutations in the spike that appear to be biologically relevant. UK scientists and epidemiologists believe that this virus is associated with increased transmission. One of the reasons is that in regions such as London and the Southern part of England, where the virus is predominant, the reproduction number rT is around 1.5 whereas in other areas it is 1.1. There’s some preliminary data which reveals that patients who have this particular mutation seem to have a higher viral load than others. But preliminary data so far doesn’t show an increase in severity or whether it is conferring escape from vaccine immunity, but definitive experiments are ongoing. Another important point is that one of these mutations in the spike protein may lead to a false negative in RT-PCR essays which target the spike gene,” he affirmed.
The South African mutation also shows a mutation in the spike protein and does seem to increase transmission and become the dominant lineage. It also shows a higher viral load in patients, but the world does not know about severity or vaccine escape.
He said that finding mutations depends on whether you’re doing sufficient sequencing to look for them. “UK is sequencing most of its COVID-19 positive samples (10%) so you have to be careful. Just because it was discovered in the UK it doesn’t mean UK is the only place having the virus. Right now we are having people coming from different parts of the world. Both these mutations and the first one are susceptible to be controlled by public health measures, but given the greater transmission potential we just need to work harder to achieve success,” he added.
Sri Lankan situation
While giving a background to the onset of COVID-19 in early March 2019, Head of Department of Immunology and Molecular Medicine at University of Sri Jayewardenepura Prof. Neelika Malavige opined that there were relatively smaller outbreaks and even a period with no cases until the Minuwangoda outbreak. “When the outbreak started in October there were two clusters ; Minuwangoda and Peliyagoda. The other important thing to understand was whether the Peliyagoda cluster was a different one from the Minuwangoda cluster and the viral sequencing told us that both these clusters developed due to the same virus which came to Sri Lanka in early September and therefore they are one cluster. SARS-COV 2 sequences identified in October and November show that the viruses are related to each other very closely, so there are no introductions from new viruses. All these viruses included in sequencing were from Kalutara, Gampaha and Colombo areas and don’t include viruses causing outbreaks in Jaffna and the northern region. Because of emerging mutations from all over the world and because we restarted tourism we have decided to sequence viruses every two weeks instead of once a month and do more sequencing.” said Prof. Malavige.

In our viruses we saw another mutation in the spike protein, but because it is not in a significant place it is not going to affect the vaccine efficacy. Other mutations aren’t significant although they are found in the non-structural proteins
Prof. Neelika Malavige
Mutations in our strains
She further said that all the viruses in the current outbreak have the 614G mutation associated with rapid spread which is not surprising because the initial virus has been replaced by this mutation. “In our viruses we saw another mutation in the spike protein, but because it is not in a significant place it is not going to affect the vaccine efficacy. Other mutations aren’t significant although they are found in the non-structural proteins. The current strain is different to the ones circulating before September and it’s the same strain that was circulating up to end of November and we haven’t found any significant mutations that affect the binding of neutralizing antibodies and therefore wouldn’t affect vaccine efficacy,” she said.
Diagnostics
Speaking about diagnostics, Prof. Malavige explained that the PCR kits in Sri Lanka target N, ORF1 or E gene. “The UK and South African mutation affects the primers that target the spike protein. So the current PCR kits in Sri Lanka have no issue with detecting the new UK strain,” she said while adding that Sri Lanka is currently conducting around 12,000 PCR tests daily.
“On the other hand, Antigen kits detect the viral Antigen, so you have to get a nasopharyngeal swab for the Antigen kit,” she continued. “But most of these Rapid Antigen kits should be read on time or else you would get a positive band. The Abbott test which is done in Sri Lanka should be read in 15 minutes. If you read at 20-25 minutes you get a faint band which you might interpret as a positive, but it is actually a false positive you get due to delayed reading. This will happen when there’s a lot of people to do Antigen tests. This is also seen in Antigen tests used for dengue,” she added.
On the other hand, a LAMP assay is a molecular diagnostic test which usually takes 30 minutes. “You can visually detect it by the appearance of fluorescence and you can use a real-time PCR machine. A highly specific and sensitive LAMP assay has been developed in Sri Lanka by SLINTEC and was evaluated in our laboratory, MRI, IDH and Karapitiya lab which has proven to be promising. If we have this test as well rolled out since it is much shorter and cheaper we can increase test capacity, especially at airports,” the professor explained.

Pricing to patients is a strange question. We normally give vaccines free, because the benefit of vaccines is the public protection. Strong economic arguments justify free pricing. Even in Australia, where they plan for private GPs to give vaccines, the vaccine itself will be free
Dr. Ravindra Rannan-Eliya
Vaccine
The AstraZeneca vaccine was approved by UK authorities and will be used soon. “But there’s a lot of concern on whether shortcuts were taken and whether the proper procedures were followed. The usual vaccine manufacturing process is where you have a pre-clinical stage where the vaccine is developed, then there are Phases 1-3 where you submit data and then only you have the authorities approving it to start the manufacturing process. But due to the pandemic situation although the pre-clinical stage was done for most vaccines each phase overlapped with other phases. Therefore, while Phase one was going Phase 2 started and while that was going on Phase 3 started and with Phase 3 the manufacturing process started as well. Manufacturing companies were also taking a huge risk because at the end of Phase 3 if the vaccine was found to be ineffective then the production would have gone to waste. All the regulatory approvals will be emergency use which is currently being given,” she added.
Who gets the vaccine and when?
Speaking on vaccine availability, she said that many infectious diseases have been wiped off or suppressed due to vaccinations and this is one of the biggest achievements. “But in this case the supply and demand are not matched and we will have to choose who will get the vaccine too. Those with comorbidites such as diabetes, cancer, cardiovascular disease and old individuals and healthcare workers who are at the frontline of treating these patients. The vaccines should be rolled out and SL has decided to immunise vulnerable groups first, but the quantity and proportion will depend on the availability of vaccines, funds and cold storage facilities. We do have cold storage facilities for the usual temperature, but if we are going for vaccines that require ultra cold temperatures then we will have to have those storage facilities in place very rapidly in order to get down those vaccines,” she explained.
Immunity and side effects
“When talking about immunity there are reports of reinfection, especially in those who have had mild infections,” she continued. “So in that case would a vaccine provide long lasting immunity and if so, for how long. The efficacy rate of the vaccines are over 90% and effective in preventing severities and symptomatic infections. But we don’t know if they would prevent transmission and/or proportion of individuals who get the illness,” she said.
She also drew attention to Anaphylaxis which is a side effect occurring in the Pfizer vaccine, especially in those who have had severe allergies. “But that doesn’t make all those with severe allergies to be excluded from getting the vaccine. If we don’t have long lasting immunity and if we can only immunise certain individuals would we have to give these vaccines on an yearly basis to high risk, vulnerable groups as we are doing with the influenza virus? Another question is the impact of emerging strains. There’s a new vaccine for influenza every year because the influenza virus, which is an RNA virus, and it changes rapidly. Will the SARS-COV-2 virus ultimately go to that extent with significant mutations causing the vaccine to be less effective? These are some questions we need to think about and only time will tell us,” she said.
Awaiting transmission blocking effectiveness data
However, according to Dr. Ravindra Rannan-Eliya, international medical researcher and Director at Institute of Health Policy none of these vaccines has or is likely to be available before mid-2021 Phase IV trial data; including adverse effects. “None have reported the ability to stop transmission, and this won’t be known till mid-2021. Since they are being approved under emergency procedures with only Phase III data, the issue of indemnity arises. Most firms will demand protection from lawsuits. Governments can provide this, and in developed countries firms will have legal protection under emergency procedures. It is not clear to me how private sellers in the Sri Lankan market would manage this or how NMRA would license. For this reason, it seems WHO approval is a must, and private distribution will need additional legal provisions.” said Dr. Rannan-Eliya
He further said that because we won’t have transmission blocking effectiveness data for some months, it is impossible right now to know which vaccine is the best. “The lowest prices will need direct Government negotiation or negotiation by COVAX. For example, EU has negotiated a much lower price on Pfizer. How this would work with private importers selling directly is an issue. There’s a host of issues nobody has thought through, especially since the Government has the right to purchase additional vaccines through COVAX at the negotiated COVAX price, and private importers will not have access to this,” he said.
“Pricing to patients is a strange question. We normally give vaccines free, because the benefit of vaccines is the public protection. Strong economic arguments justify free pricing. Even in Australia, where they plan for private GPs to give vaccines, the vaccine itself will be free,” he added.
“My own view is that if we cannot vaccinate everyone for free because the Government lacks money, we should allow private sellers to access vaccines at the lower COVAX price through the COVAX Government window, and then sell on, but impose a levy to recover the implicit cost of the insurance that the Government will need to provide against adverse effects, plus charge additional to help the government to distribute the vaccine to additional people in the public scheme,” he added.
When asked what the Government should do in the case repeated doses of the vaccine are required, Dr, Rannan-Eliya pointed out that most individuals only require two doses. “However, we don’t know how long immunity will last, so revaccination every year might be needed. For this reason and the cost, the plan should be to achieve zero virus now through effective control policies, such as investing in testing, etc. Then wait and see till the clinical trial data are clearer about ability to block transmission, and prices are falling. Then pick the most cost-effective vaccine in late 2021 or 2022, and negotiate pricing, and vaccinate everyone. In the meantime, we should think carefully about which vaccine we want for free from COVAX (20% coverage), and then use this for targeted vaccinations,” he added.
Ranaweera Tuesday, 12 January 2021 02:32 PM
Vaccine is the best option. Testing negative does not mean that the person has no virus afterwards. He may have got it from the testing center.

Add comment
Comments will be edited (grammar, spelling and slang) and authorized at the discretion of Daily Mirror online. The website also has the right not to publish selected comments.
Reply To:
Name - Reply Comment

US authorities are currently reviewing the manifest of every cargo aboard MV

On March 26, a couple arriving from Thailand was arrested with 88 live animal

According to villagers from Naula-Moragolla out of 105 families 80 can afford

Is the situation in Sri Lanka so grim that locals harbour hope that they coul